


Fatty liver disease has a weight problem — not in the way most people think.
The condition is so consistently associated with obesity in public health messaging that a person with a normal BMI who receives a fatty liver diagnosis on an ultrasound will often be told, directly or indirectly, not to worry too much. They are not the typical patient. Their weight is fine. It probably looks worse than it is.
The evidence says otherwise. And in India specifically, the evidence says this assumption may be doing real harm.
What MASLD Is — and Why the Name Changed in 2023
Fatty liver disease was known for decades as NAFLD — Non-Alcoholic Fatty Liver Disease. In June 2023, an international consensus involving over 236 experts across 56 countries, led by the major hepatology societies of America, Europe, and Latin America, renamed it MASLD: Metabolic dysfunction-Associated Steatotic Liver Disease.
The name change was not cosmetic. It reflected a fundamental shift in how the condition is understood.
The old name defined the disease by what it wasn’t — not caused by alcohol. The new name defines it by what it is: driven by metabolic dysfunction. The five cardiometabolic risk factors that now define MASLD — excess weight or waist circumference, high blood sugar or insulin resistance, high blood pressure, high triglycerides, or low HDL cholesterol — place metabolic health at the centre of the diagnosis, not body weight.
This matters because a person with normal body weight can have insulin resistance. Can have high triglycerides. Can have central adiposity that a BMI calculation will never detect. Under the NAFLD framework, weight was the primary signal. Under MASLD, it is one of five — and not necessarily the most important one.
MASLD is now the most common chronic liver condition in the world, affecting an estimated 38% of the global adult population. In India, estimates range from 16 to 32% of the population — approximately 120 million people. A 2024 analysis using the Global Burden of Disease database found that India carries the highest MASLD-attributable disease burden of any nation studied.
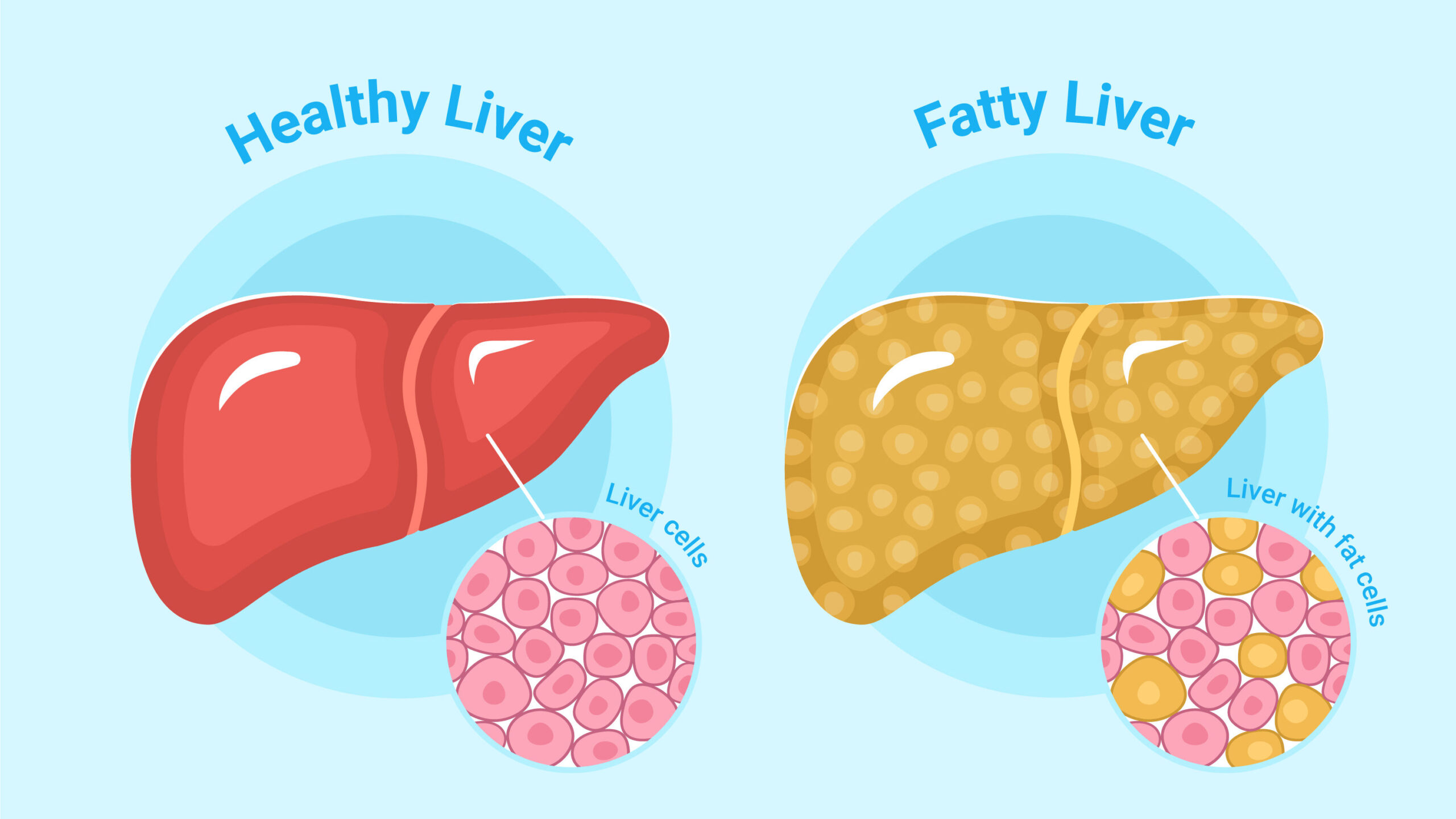
The Lean Paradox: Fatty Liver Without Excess Weight
Approximately 14–17% of Indian patients diagnosed with MASLD have a completely normal BMI. A biopsy-based study of lean liver donors in India — people who by definition underwent rigorous health screening — found that 33.7% had MASLD. These were not sick individuals with known liver disease. They were people healthy enough to donate a liver, with normal weight, whose liver tissue showed evidence of metabolic dysfunction-associated steatosis.
This is the lean MASLD paradox: the absence of obesity does not reliably indicate the absence of fatty liver disease.
The mechanism involves visceral fat — fat stored around and within internal organs rather than subcutaneously under the skin. Visceral fat is metabolically active in a way that subcutaneous fat is not. It releases inflammatory signals, promotes insulin resistance, and directly contributes to fat accumulation in the liver. The critical distinction is that visceral fat accumulation does not require high total body weight. It can occur at normal or even low BMI, particularly in populations with a genetic predisposition toward central fat storage.
Indian populations are one such group. Decades of research have documented that Indians accumulate visceral fat at lower absolute body weights than European populations — a characteristic linked to both genetic factors and early developmental influences. The result is a phenotype researchers now formally describe as “metabolically obese normal weight” (MONW): a person whose BMI suggests metabolic health, but whose fat distribution and metabolic markers tell a different story.
A 2025 review published in Frontiers in Nutrition specifically characterised the Indian lean MASLD phenotype, noting that lean MASLD patients in India show markedly abnormal metabolic profiles — dyslipidaemia, impaired glucose metabolism, and central adiposity — comparable to those seen in obese MASLD patients, despite their normal weight.
Why Lean MASLD Is Clinically More Dangerous — Not Less
This is the finding that most disrupts the conventional assumption.
A 2025 meta-analysis published in Frontiers in Gastroenterology, reviewing data from 94,181 MASLD patients, found that lean MASLD patients had a 1.6-fold higher risk of all-cause mortality compared to non-lean MASLD patients. Liver-related mortality was 1.88 times higher in the lean group.
Why would a thinner patient with fatty liver disease do worse than a heavier one?
Several explanations have been proposed. Lean MASLD may represent a more aggressive disease phenotype driven by distinct biological mechanisms — specifically genetic variants like PNPLA3 that promote liver fat accumulation independently of metabolic syndrome. These variants appear more prevalent in lean MASLD cases. Additionally, lean patients are less likely to be screened, less likely to receive a diagnosis early, and less likely to be placed on surveillance protocols — because the weight-based risk signal is absent. The disease progresses undetected for longer.
There is also a survivorship dynamic at play. Obese patients with MASLD often have multiple comorbidities — cardiovascular disease, diabetes, hypertension — that are being actively monitored and managed. Lean MASLD patients may have fewer of these comorbidities flagged, receive less metabolic monitoring overall, and have the liver disease identified later in its course.
The 2023 PGI Chandigarh study of 1,040 NAFLD patients confirmed this in the Indian context: lean patients showed similar liver disease severity on biopsy to non-lean patients, despite having fewer metabolic risk factors. The liver was equally affected. The clinical attention was not.
The Progression Nobody Sees Coming
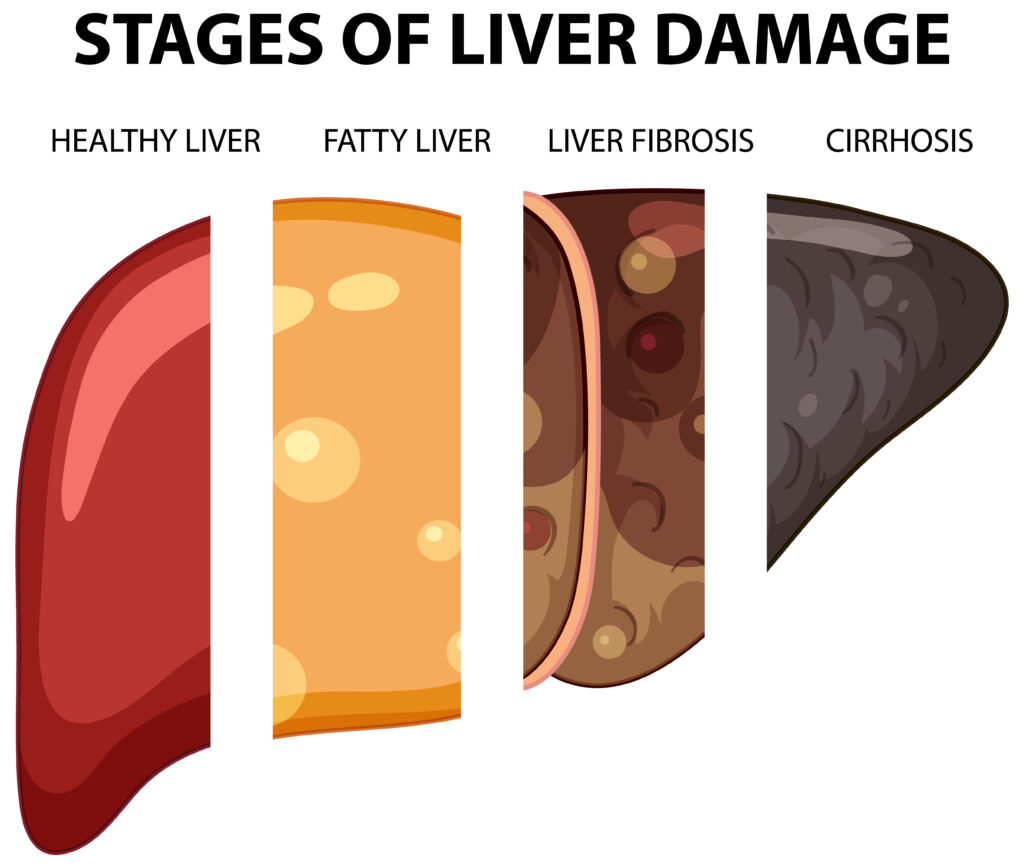
MASLD exists on a spectrum. Simple steatosis — fat in the liver without significant inflammation — is the earliest stage and is generally reversible. A meaningful proportion of patients progress to MASH (Metabolic dysfunction-Associated Steatohepatitis), where fat accumulation is accompanied by liver cell inflammation and injury. From MASH, a subset progresses to fibrosis — scarring of liver tissue — and ultimately cirrhosis, where scarring is extensive and liver function is irreversibly impaired.
The critical problem is that this entire progression — from steatosis to early cirrhosis — is almost completely silent. There are no reliable symptoms at the early and intermediate stages. Fatigue and mild right upper abdominal discomfort occur in some patients, but these are non-specific and frequently attributed to other causes. Most people with MASLD, lean or otherwise, have no symptoms until the disease is advanced.
This is why incidental detection on ultrasound — performed for an unrelated reason — is the most common route to diagnosis. The question is what happens next. A finding of “mild fatty liver” on an ultrasound report, handed to a patient without follow-up context or metabolic assessment, frequently results in no further action. For lean patients especially, the assumption is that the finding is benign.
It may not be.
Who Is at Risk Beyond the Obvious
The standard risk profile for MASLD — overweight, diabetic, metabolically unwell — captures the majority but misses a substantial minority. For Indian patients specifically, the following should prompt assessment regardless of BMI:
Central adiposity without obesity. Waist circumference above 80 cm in women and 90 cm in men — the Asian-specific cut-offs — in the presence of normal BMI is a recognised risk signal for visceral fat accumulation and metabolic dysfunction.
Family history of liver disease, diabetes, or metabolic syndrome. Genetic variants influencing liver fat accumulation are heritable. A first-degree relative with fatty liver disease, cirrhosis, or early-onset diabetes substantially increases individual risk.
Incidental ultrasound finding. Any ultrasound report noting hepatic steatosis — regardless of severity classification or the patient’s weight — warrants metabolic evaluation rather than watchful waiting.
Abnormal liver enzymes without clear cause. Elevated ALT or AST in a lean patient without alcohol use, viral hepatitis, or medication history should raise MASLD as a differential diagnosis rather than being dismissed as isolated findings.
Insulin resistance markers. Fasting glucose in the pre-diabetic range, elevated triglycerides, or low HDL in the absence of other explanation are metabolic signals that warrant liver assessment.
What Assessment and Management Look Like
A complete assessment for suspected MASLD in a lean patient includes liver enzyme levels (ALT, AST, GGT), fasting glucose and insulin, lipid profile, and ultrasound or controlled attenuation parameter (CAP) measurement for steatosis. For those with evidence of disease, non-invasive fibrosis assessment — FIB-4 score or liver stiffness measurement — stratifies progression risk without requiring biopsy in most cases.
Management in lean MASLD follows the same principles as in obese MASLD, with important modifications. Weight loss targets are less applicable — and in lean patients, aggressive caloric restriction is neither safe nor appropriate. The focus shifts to metabolic optimisation: insulin sensitivity, lipid management, physical activity to reduce visceral fat specifically (resistance training and aerobic exercise both reduce visceral adiposity independently of scale weight), and dietary quality rather than quantity. Refined carbohydrates, fructose, and ultra-processed foods drive hepatic fat accumulation in lean individuals through the same insulin-resistance mechanisms as in obese patients.
Regular monitoring — liver enzymes and non-invasive fibrosis scoring at intervals determined by disease stage — is essential. Lean MASLD patients should not be discharged from follow-up because their weight is normal.
The Bottom Line
Fatty liver disease is a metabolic condition. Body weight is one of its drivers. It is not the only one — and in India, where visceral fat accumulation at normal weight is well-documented and common, it may not even be the most reliable indicator.
A normal BMI in a person with MASLD is not a protective factor. The outcomes data suggests it may be associated with worse prognosis, partly because of disease biology and partly because the weight-based risk framework fails to trigger the clinical attention these patients need.
The liver does not read the BMI chart.
📚 References:
Dey P. Frontiers in Nutrition, 2025.
GBD 2021 Analysis. PubMed Central, 2024.
De A et al. International Journal of Obesity, 2023.
Wongtrakul et al. Frontiers in Gastroenterology, 2025.
Chakrabarti SK et al. Science Frontier, 2025.
Rinella ME et al. Journal of Hepatology / Hepatology, 2023. (MASLD nomenclature consensus)
For assessment of liver health, metabolic risk, and related concerns, SDDM Hospital’s Gastroenterology and Internal Medicine departments are available at +91-191-2464637 or sddm.hospital.
This article is for general educational purposes and does not constitute medical advice. Please consult a qualified healthcare professional for individualised assessment and guidance.
SDDM Hospital, Jammu Multi-Specialty Care | Gastroenterology | Internal Medicine 📍 Channi Himmat, Jammu | 📞 +91-191-2464637 | 🌐 sddm.hospital